あなたはいつもドライアイ病気について知りたかったこと...そして決して尋ねることはありませんでした!
詳しくは
約
ドライアイ病
---ドライアイ疾患の事実...ドライアイ疾患の原因
...ドライアイの治療
...ドライアイ病に対して何ができますか?
...ドライアイの治療...

あなたはいつもドライアイ病気について知りたかったこと...そして決して尋ねることはありませんでした!
---ドライアイ疾患の事実...ドライアイ疾患の原因
...ドライアイの治療
...ドライアイ病に対して何ができますか?
...ドライアイの治療...

すべてのドライアイが正しく認識されるわけではありません 。なぜなら、症状はしばしば特徴的で はなく、発症はしばしば忍び寄るからです。
ほとんどの苦情 ドライアイ疾患ではで説明されているの刺激 目と涙液膜の乱れ :
これは、「疲れた目 」、「重い瞼」または「膠着した目」に つながります
ドライアイの痛み は、異なる領域で起こり得る:
持続的な眼の刺激は痛みにつながり、慢性的な痛みは疼痛症候群につながる可能性があります。 慢性疼痛症候群は、ドライアイ病の明確な疾患要因であり、しばしば治療が困難である。痛みのある薬や心理療法とのコラボレーションがここで役立ちます。
ドライアイ疾患では、良好な視力に重要な均一な薄い涙液膜が乱されます。そのため、 多くの患者が視力持っている ような問題を
治療は =>ドライアイにおける視覚障害は、一般的に向上させる、またはさえ消え、新たな安定した涙液層を広げる一つまたは複数の強力なまぶたが点滅し、後に、一時的に。 - これは、視覚障害が涙液膜障害によるものかどうかの良いテストです。
治療 =>ここでは、眼科医による精密検査と小手術が有用かもしれません。
濡れた目のための他の理由と 蓋の縁の上の涙は:
まぶたの形や位置が変更されたときに、涙液膜が適切に形成されなくなったり、眼に保持できなくなったりする... 鼻への涙の流出が 眼から少し離れて傾いているか、排液している涙管の閉塞のために正常に機能しなくなったとき。
涙液膜は何から成っていますか?- 眼の腺からの分泌物のうち!
涙のフィルムはどのように作られていますか?- まぶたが涙のフィルムを広げた!
涙のフィルムはどこに行きますか? - 涙が鼻に流出する!


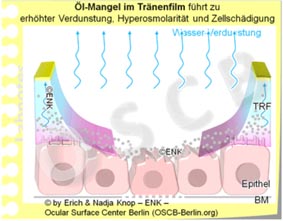
水分の欠如は、しばしば 、涙腺を通る水分涙の産生の減少によって引き起こされると考えられている。しかし、涙腺の障害による水の主要な欠乏は非常にまれである。
眼の表面上の涙水の 蒸発の増加による(2次的)水分損失がずっと一般的である。これは油の欠乏の場合に起こり、環境の影響を取り除くことによって悪化する。
涙液膜の欠損は、蒸発の増加に起因するか、または原発性低涙腺生成によるかにかかわらず、眼表面に組織損傷を引き起こす
治療が => 水性点眼剤の有無にかかわらず、添加油、有用な治療法です。
...それらは必要に応じて、しばしば十分に、1時間に1倍まで使用されるべきです。水性点眼剤をさらに頻繁に使用することは、通常、有用ではありません。これは、自分自身の(残余)涙の影響を減らすことができ、それによって眼の刺激が悪化する可能性があるからです。
ほとんどの場合、涙の水が最初に欠落するのではなく、水の蒸発を減少させる涙膜の油の表面層です。
油の欠乏は、通常、眼瞼のマイボーム腺の障害によって引き起こされる 。腺が詰まると、油がなくなり、水分の涙がより速く蒸発し、目が乾燥します。 マイボーム腺疾患は非常に一般的であり、年齢とともに増加する 。
治療 =>油や脂質スプレーが含まれている点眼薬はここで助けることができます...しかし...
...とりわけ、眼瞼の油産生マイボーム腺の機能を再び改善することが重要 です!これは 、患者が自宅で定期的に行い、腺の閉塞および損傷を改善する物理的な瞼治療(温暖化、マッサージ、クレンジング)によって行われる。
「Bリンク」と呼ばれる通常のまぶたのストライクは、内部のまぶたの筋肉の動作によって実行され、必要です。
まれな 点滅 および 不完全な 点滅 は、涙液膜欠損の一般的な原因である。
Office Eye / Office Eyeは、近代的なオフィスワーク環境で急速に成長するドライアイの一形態です 。これは、いくつかの有害な影響を追加し、ドライアイに速くつながります。このようなドライアイの形態は、高齢者に影響するだけでなく、若年層でもより 頻繁に発生する 。
コンピュータ、テレビ、運転などの集中した視覚的作業はまれな点滅 を伴うため、容易に乾いた目につながり ます。
ドライアイの危険性が増しています。
不安定な涙液膜に加えて、まだ乾燥している環境要因とおそらくは涙液生成に対する負の内部影響が加わる。
治療 =>十分に頻繁かつ完全なまぶたのストライキのために、私の観察と、必要であれば、まぶたの変化が重要です。さらに、意図的な点滅の演習 覚えても、コンピュータのアプリがある-仕事では便利です。さらに、作業環境を乾かすことを避け、十分な休憩と十分な飲酒量が役立ちます。
涙障害は、眼表面の刺激を誘発するか、または悪化させる。
刺激された眼球表面は、次に、損傷した眼球表面上の涙液膜の安定性を悪化させる。
涙液不足症および眼球表面組織損傷は、明らかに、「悪循環」と呼ばれるものによってリンクされています。ここでは、機能不全が他のものを悪化させ、開始イベントを補強します。
したがって、ドライアイ疾患は、 十分に治療されなければ、それ自体が悪化する傾向がある。
治療 =>有害な自己悪化(Vicious Circles)の中断は次のようにして行うことができます:

眼球表面が永続的に炎症を起こしている場合、典型的にはドライアイでは炎症反応を引き起こす可能性があります。炎症は実際には眼の防御である。しかし、炎症が永続的に起こる場合、それはドライアイの自己悪化を増加させる可能性があります。
THERAPY =>ここでは、抗炎症療法眼科医によっては有用である可能性があります。
あなたが信頼する眼科医、そして重度の症例では、専門のシッカセンターでさえ、さらに多くの治療法があります。


偉大な旅の始まり...友達と
あなたのSTARTにぴったりで、トピックへの浸漬に最適なOSCB情報WebSite の国際凝縮バージョンへようこそ!
より詳細な情報参照してくださいオリジナルフルレングスの英語言語バージョン
ホームページのメインメニューのTOPICSにアクセスしてください
これらの異なる、そして部分的に矛盾して現れる苦情はすべて 、眼の表面組織の損傷のために起こる眼の炎症の症状であり得る
これは典型的に目の前の涙液膜の不足に続いて起こります。それは、もはや繊細な組織を十分な湿った状態に保つことができなくなります... 組織が乾燥する結果 - これが「ドライ アイ」という言葉の背後にある理由です
「乾燥」という用語とは対照的に、眼の表面組織の発生する刺激は、過剰な引き裂き および水まきのエピソードを招く可能性がある。これは特にこの状態の初期段階で起こり、患者にとって理解することが困難なことが多い。
水を注ぐ場合の涙液量の増加 は、(まだ)完全な保護涙反射を示し得る。この反射は、一般的に、風やファンなどの多くの種類の刺激や異物などによって引き起こされます。そのような刺激的な出来事は刺激を取り除くために涙を流す。ときに眼表面の損傷進み、この保護反射は不幸にも機能不全になると消えます。まぶたの境界上に涙液が溢れている目に水をまき散らす別の理由は、眼瞼変形のために起こることがあります。眼瞼変形を伴う眼は正常な涙液膜を形成することができないか、または眼表面に保持することができないため、これらの状態は眼の炎症を伴うドライアイ疾患につながる。頻繁な眼瞼の変形は、例えば、進行中の年齢の組織変化に典型的に生じる眼瞼縁(内棘または隆起)の内向きまたは外向きのねじれである。
これらのいくつかの熟考は、いわゆる「DRY EYE」病気が予期しないトリッキーな問題であることをすでに示している。
「トリッキー」は、「ドライアイ病」の目が水になることができるという事実だけではありません。
トリッキーはまた、驚くべきことに... 「ドライアイ」の病気の患者のほとんど は水分が一切欠けていませんが、涙液には油分が一番欠けています。
涙液膜の表面のオイルは、涙水の蒸発を遅くする機能を持っています...暖かい水が入った鍋の蓋に似ています。
眼表面の健康機能が依存する要因が多数ある相互関連および相互依存。
眼球表面の機能的および構造的ネットワークはおそらくカードハウスと比較されるかもしれません - 安定しているように見えますが、カードが1枚移動するとすぐに...
科学は、目の病気の解決に取り組んでいます。そのうちの1つはドライアイが最も頻繁に起こります。世界中の研究者は知識のかなりの進歩を遂げました。
ドライアイ病に罹患している世界中の何億人もの患者さんの日常生活に役立ちました。
しかし、将来の治療のためのより効果的な戦略を提供するためには、病気のプロセスへのより深い洞察とそれに続く科学的進歩が必要です。
患者のために重要なのは、有益な方法で状態に影響を及ぼす多くの方法を理解するために、彼/彼女の状態を理解することです。
...顎顔面センターベルリン(OSCB)の顎顔面および乾燥眼病に関する情報プラットフォーム - 眼科表面および眼瞼乾燥症に関する知識の向上のための非営利科学研究所 フィールド内の経験豊富な科学者によって。
味のあるページを選んでください。




Choose your CHAPTER of Interest - or simply read along ... which may be most instructive
The shining of the Ocular Surface comes from the Tear Film ...
... that maintains the permanent Moisture of the Ocular Surface.
Moisture is necessary for the health of the ocular surface tissue and moisture is also important for perfectly clear vision.
Without sufficient moisture the vision becomes blurry, the tissue is increasingly damaged, and sensations of discomfort occur.
The OCULAR SURFACE is that part of the eye that permits the entrance of Light.
Only after passing the Ocular Surface
... can this light elicit responses of the Retina in the back of the eye
... that later allow the ´curious´ Brain to construct an image of the outside world on the screen of consciousness.
Without a healthy and functioning Ocular Surface, all other steps of the Vision Process that happen later and further ´behind´ ... are basically meaningless.
Our Ocular Surface has the biological requirement that it must be permanently moist - ´always and everywhere´ - to keep the transparent window of the cornea indeed clear.
The Moisture is produced by the associated Glands of the Ocular Surface and it is termed as the ´Tears*.
Since we are living in a dry environment with an air atmosphere, it is actually quite laborious to preserve this little artificial moist ´ecological niche´ of the Ocular Surface - ´always and everywhere´ !
PS: * except for moistening the Ocular Surface, Tears are also of use to give the emotional signal to our fellow human beings that we are exceptionally sad ... or probably exceptionally happy by shedding ´tears of joy´
The Tear Fluid is produced by several Ocular Glands.
There are three different types of glands needed, because the tear film on the eye consists of three different types of substances.
Tears are produced by the various Glands at the Ocular Surface.
The bulk volume consists of water and comes from the lacrimal gland that is located upstream in the upper lateral side of the bony orbit.
From there the tears enter the conjunctival sac. They are flowing over the visible anterior part of the eye and thus constantly bathe this area.
At the nasal side the ´used tears´ are sucked up by two narrow lacrimal puncta, one at each nasal end of the upper and lower eyelid.
Through the lacrimal drainage system the tears enter the nose. When tears go there in larger quantities, e.g. in emotional crying, they may flow backwards into the pharynx where we can sense their salty taste.
Meibomian oil protects the tear water from evaporation.
The Meibomian glands produce lipids that are liquid at body temperature and thus form an oil.
The glands are of particular importance for the health of the ocular surface because their oil retards the evaporation of the tear water from the lacrimal glands.
In the dry environment that we live in, even a copious secretion of tear water would rapidly evaporate from the ocular surface if it was not protected by the superficial Meibomian oil layer on the tear film.
The Meibomian glands form individual long bodies that fill the tarsal plates of our eyelids. About 25-30 glands can be found in every healthy eyelid and the little orifice is close onto the posterior lid margin ... as can be seen in an ordinary mirror, by everybody who is interested.
With every blink of the eyelids a little drop of oil is expressed by the lid muscle. It gets from the gland onto the eyelid margin and the tear film. where it protects the aqueous tear film from too rapid evaporation.
The requirement of Moisture - ´always and everywhere´ - confronts the ocular surface with a problem or, more positively thinking, this gives it the change to deal with a Challenge:
Light can only enter the eye when the eyelids are opened ...
... on the other hand, opening of the eyelids would at the same time immediately deprive the Ocular Surface tissue of its moisture and it would start to dry out.
To solve this Dilemma, the Ocular Surface has to apply a ´Trick´: A very narrow layer of fluid is formed from the tears - this is for obvious reasons termed as the Tear Film.
The Tear Film is thick enough to preserve the moisture for the underlying cells of the tissue but not too thick in order not to harm the transmission of light.
The Ocular Surface in fact manages to be even more ingenious, because it solves the dilemma by even improving the passage of light through the presence of the Tear Film. The Tear Film fills in all subtle inequalities of the ocular surface and thereby provides a perfectly Smooth Surface layer for perfect refraction of the incoming light that allows for perfect Visual Acuity.
The Tears are transformed into the thin, homogeneous Tear Film ... through the coordinated Movement of the Eye Lids - the BLINK.
During the blink mainly the upper eye lid wipes over the anterior surface of the eyeball and thus distributes the tears into the very narrow Tear Film.
During the down-phase of the blink the old tear film is removed by the upper eyelid and during the up-phase the upper eyelid draws out a new intact homogeneous tear film.
It becomes obvious that any disruption of the EyeLid and of their normal Blink movement and speed is an important factor for the onset on a Dry Eye condition . This is termed as ´Eyelid and Blinking Disfunction´ (abbreviated as LBD).

Only through the coordinated blink movement of the eyelids, together with the very special composition of the Tears , is it possible to form a TEAR FILM that is extremely thin (only about one hundreds of a millimeter).
At the same time this very narrow tear film must still be stable to allow the curious brain to achieve a sufficiently sharply focused image of the outside world.
The Tear Film must be stable for at least 10 seconds on average until it eventually breaks up and triggers a stimulus that induces a new blink that forms a new tear film.
Having said this ... all major things are basically named ... The basic functional pre-condition at the ocular surface for vision is a Stable Tear Film. This is achieved by the Basic Functional Complexes of Tear Secretion/ Production by the ocular glands and of the physical Tear Film Formation by the blink movement of the eyelids.

The formation and preservation of the Tear FILM is very laborious in the dry environment that we live in, and is thus very vulnerable.
The Tear Film depends on a multitude of very different Influence Factors, that can, in one or the other way, have a positive or negative influence.
All negative influence factors are Risk-Factors - they can, sooner or later, lead to a Dry Eye condition - particularly when they become chronic.
The large number of influence factors that may appear unrelated at first glance can let Dry Eye Disease appear as a ´Tricky Condition´ - even though it basically straightforward.
The Tear Film has the function to prevent Drying of the Ocular Surface Tissue. Therefore the most immediate consequence of a Dry Eye condition is typically the Drying and thus Destruction of the Ocular Surface Tissue.
The eye lids can then often be sealed by sticky mucus and encrustations.
This results in a ´downstream´ irritation of nerve fibers They transmit ocular irritation of various degrees and can lead to pain that is often described on and around, occasionally behind, the eye. Inflammatory reactions can reinforce the whole process, eventually leading to severe tissue destruction and to a chronic pain syndrome.
Since the Tear Film also has an important function for the refraction of light and thus for the provision of visual acuity, it is no surprise, that visual disturbance is frequently reported in Dry Eye Disease, typically in terms of unstable visual acuity and blurred vision
According to the present scientific knowledge, the vast majority, i.e. four of five patients with a Dry Eye Condition, does NOT have a primary lack of water but instead a PRIMARY LACK OF OIL in the tear film.
This leads to increased water evaporation and decreased tear film stability .... with a secondary water loss.
Therefore, in most patients, it does not seem to make much sense nowadays to use products that do not contain lipids in one or the other way.
It may be possible to replace the effect of lipids on the tear film by other compounds, or to simply use lipids only, e.g. as a liposomal spray. ... In other words, LIPIDS or respective compounds should nowadays be a component of a typical Tear Supplementation Therapy.

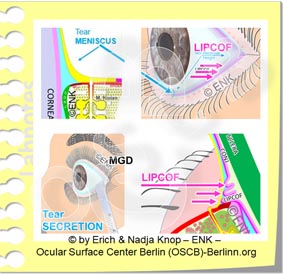
The lack of oil on the ocular surface is typically due to Meibomian Gland Dysfunction (MGD), a mostly obstructive condition of the Oil-producing little glands inside the eye lids.
The glands are blocked by inspissated secretum and excessive keratinization - therefore inspissated oil accumulates inside the glands.
Muscular force during blinking of the eyelids normally helps to express the oil from the Meibomian glands.
Rare Blinking is thought to be an important factor for a lack of oil on the tear film and possibly a co-factor for onset of gland dysfunction.
Intended forceful blinking is known as a simple way to increase the oil layer on the tear film and thus to improve tear film stability in order to prevent ocular surface dryness.
In most cases there is a deficiency of the Tear FILM based on a qualitative or quantitative lack of Tear Components.
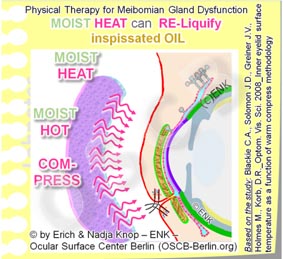
Physical Eyelid Therapy options refer to the fact that the improvement of Eyelid and Meibomian Gland Disease is based on simple but effective physical techniques such as Warming and Moistening, as well as manual Massage and Expression of the Glands with subsequent Scrubbing and Cleaning of the Eyelid Margin.
It is certainly important to note that before any manipulations are done to the eyelids and the eye a clinician should always be consulted for an educated diagnosis and for therapeutic recommendations !
It appears necessary that Physical Therapy is done as a permanent therapy, at best twice a day - because a chronic disease typically requires a chronic therapy. Only a chronic consequent therapy is able to improve the disease condition - still, there is typically only a slow but steady improvement !
In order to achieve 40°C inside the eyelid a slightly warmer (42-45°C) moist warm compress/ cloth must be rewarmed (e.g. from a larger bowl of hot water) every two minutes as shown by studies.
The additional moisture serves to soften up the cornified epithelial squames and lipid encrustations on the eyelid margin.
Commercially available gel masks or even electrically heated and moistened googles may make the potentially laborious effort of physical therapy, twice a day, considerably easier ...
The advantage of such physical therapy options is certainly, that this can mostly be done at home by the patients themselves. It may appear as a disadvantage that physical therapy and in particular lid hygiene has to be done routinely once or twice a day, similar e.g. to tooth brushing, but requires slightly more time.
... or, to re-phrase it in the Roman way: ´palpebra sana in corpore sano´ - unproven quote from Clarissimus GALEN ;-)
- - -
Various other THERAPY OPTIONS are discussed in other Chapters of the full length English Language Pages of the OSCB Information WebSite.
Contact Lenses are a fantastic Optical Tool with some clear optical advantages compared with spectacles.
At the same time they provide greater ´freedom´ for outdoor activities, sports and society events.
Contact Lenses are, as their name indicates, in direct ´contact´ with the Ocular Surface.
Contact Lenses are in fact sitting in the middle of the Ocular Surface Functional Unit - with potential influence on all tissues and on the tear film.
Contact Lenses thus have a somewhat ambiguous role for the Ocular Surface - with Pros and Cons.
Contact Lenses can be used for medical purposes such as the optical correction of an irregular corneal shape or for the protection of the eye e.g. in severe cases of Dry Eye Disease.
On the other hand, Contact Lenses have higher ´requirements´ for the amount and/or quality of the tear film.
It may well be, that an individual with a borderline normal tear film, who is still without symptoms, may develop Dry Eye symptoms upon insertion of an ordinary soft hydrogel contact lens.
A typical side effect of Contact Lenses is therefore the onset of Dry Eye symptoms and eventually probably of Dry Eye Disease.
On the other hand an individual with a severe Dry Eye Disease may profit from the application of a special so-called ´Scleral´ Contact Lens that is able to preserve the tear solution underneath the contact lens and in front of the cornea.
Contact Lenses have seen great improvements in the past decades.
This has lead to a reduction in the frequency and severity of side effects.
Insufficient Hygiene can lead to serious and sight-threatening infections in contact lens wear.
This is still an important issue, particularly for inexperienced wearers.
Due to the increasing use of disposable contact lenses for short term wear, particularly daily disposables, the risk of infection can be reduced.
Please find more information below on => Contact Lenses and the Ocular Surface

Choose your CHAPTER of Interest - or simply read along ... which may be most instructive


The OCULAR SURFACE is the moist tissue at the anterior side of the eye ball
Moisture is necessary to preserve its health and integrity - and it is thus a pre-requisite for VISION.
The Glands of the Ocular Surface for the production of the dfferent components of water, oil and slime/mucus together form the tear fluid.
The Tears are the essential medium for the provision of moisture at the Ocular Surface.
The Eye Lids spread the tears into the essential pre-ocular Tear Film.
The Tear Film makes it possible that moisture can even persist on the tissue within the opened palpebral fissure. In addition to moisture the Tear Film aids in allowing a perfect light refraction and thus a perfect vision at the same time.
The Healthy Ocular Surface is a Pre-Requisite for Vision and without it all later steps of the vision process are meaningless.
DRY EYE DISEASE is medically also addressed as ´Keratoconjunctivitis Sicca´ - which means ´dry inflammation of the cornea and conjunctiva´ or only as the ´Sicca Syndrome´ (bunch of symptoms related to dryness) . This condition has various colloquial names such as simply ´dry´ eyes, ´ocular dryness´, ´itchy eyes´´heavy lids´ or ´tired eyes´ etc.
Dry Eye Disease typically shows the two PATHOLOGIES of
The basic CAUSATIVE FACTORS for Dry Eye Disease are those that directly lead to the deficiency of the Tear FILM - this is
Such patho-physiological analysis of the disease process in Dry Eye Disease led to the ´Holistic Dynamic Concept´ of Dry Eye Disease as described in the Dry Eye Chapter of the original full length English language version of the OSCB WebSite.
The main clinical signs of Dry Eye Disease are thus:
Instability of the Tear Film is a typical feature of any type of Dry Eye Disease and thus important to be investigated.
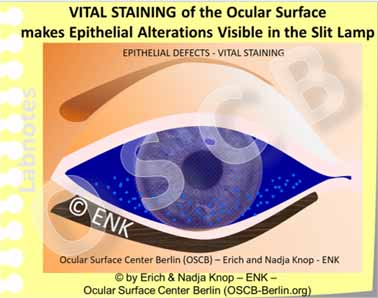
Vital staining is a quick and easy way to verify another important feature of any type of Dry Eye Disease which is alteration, wounding and destruction of the normal epithelial structure
Tear Film Deficiency and Surface Damage lead to typical subjective irritative SYMPTOMS of the patient.
Typical Syptoms in Dry Eye Disease are e.g. ocular irritation, dryness and grittiness, often described as ´heavy eye lids´ or ´tired eyes´, together with an unstable visual acuity and episodes of blurred vision, with various degrees of irritation and pain.
Initially the ocular irritation due to tissue alterations can lead to episodes of increased tearing, watery eyes and tear dripping over the lid margin.
The ONSET and PROGRESSION of Dry Eye Disease is strongly influenced by many different factors.
An often underestimated Risk Factor for the promotion of Dry Eye Disease is various types of medication. This is true in addition to the potential negative influence on ocular heath that may come from the presence of systemic disease as such, that may require the medication.
Pharmacological therapy may promote the onset or progression of Dry Eye Disease when they change the internal milieu of the body in a way that has a negative influence on the production of tear components. Another issue occurs when they have a direct negative influence on the health, vitality and integrity of the ocular surface. The latter can occur e.g. in malnutrition of e.g Vitamin A, and in chronic inflammatory ocular surface disease as e,g, in Graft versus Host disease (GvHD) that as typically observed after bone marrow transplantation.
The medicine-related and often pharmacological negative influence on the health of the ocular surface and on the promotion of Dry Eye Disease was in the recent (2017) TFOS DEWS II Report designated an own type of disease, the ´Iatrogenic Dry Eye´.
Many classes of pharmacologicals are known or supposed to promote Dry Eye Disease. This includes, e.g.
The potential promotion of dry eye disease depends, however, on the actual medication and on the dosage. An intended necessary positive drug effect on the disease in question certainly has to be weighed against a potential unwanted side effect in order not to endanger the health of a patient. Generally, a medical therapy that is advised by a doctor should not be changed of removed by a patient without better knowledge !
A direct damage of the ocular surface occurs in particular by the chemicals that are added to eye drops as a preservative in order to prolong the shelf-life and their time of usage by the patient.
This is a problem in particular when the eye drops have to be applied frequently or regularly as in tear supplementation therapy and topical glaucoma therapy.
Frequent application of preservatives often leads to a considerable damage of the fine structure of the ocular surface and thus to decreased wetting of the tissue and to instability of the tear film.
Luckily many eye drops are available today in a preservative free form either in small Single Dose Containers or in sterile drop dispensing bottles. Whenever possible such preservative free medication should be preferred.
in Dry Eye Disease are
Tear Film Deficiency and Surface Damage influence each other negatively and are therefore linked by several self-enforcing vicious circles that lead to worsening of the condition.
are a typical component of Dry Eye Disease because inflammation represent a basic protective mechanism of wounded tissue - and this is also true for the Ocular Surface.
When the wounding becomes chronic the inflammatory answers of the tissue also become chronic and more severe.
Inflammatory pathways are thus an important disease mechanism for worsening of the condition in chronic ocular surface disease.
Occasional ocular DRYNESS can certainly occur once in a while also in healthy individuals. Such dryness typically depends on adverse environmental factors, is short-lived and disappears quickly after some vigorous eye blinks or when the negative factors are removed. When the condition becomes chronic, however, an occasional ocular dryness can turn into a manifest permanent Dry Eye DISEASE.
Contact Lenses are a fantastic Optical Tool that has long been desired by many individuals with refractive disorders.
They became eventually widely usable only in the second half of the 20th century and have seen great.improvements since then.
´Rigid´ Contact Lenses are typically smaller and exclusively rest on the cornea. They need a certain adaptation time for the wearer and are thus less widespread, but have superior inert material and optical quality.
Contact Lenses can correct refractive errors directly on the cornea and therefore, they have some principal optical advantages compared to spectacles.
Contact Lenses certainly provide greater ´freedom´ for the user in a lot of sporting, outdoor and society activities.
There are different basic types of Contact Lenses. Soft hydrogel Contact Lenses are the most widely used type.
Soft lenses can typically be worn without distinct irritation and thus often require no adaptation time for the wearer to get used to a lens.
This may be a reason why most Contact Lenses are of the ´Soft´ type and are not worn for medical but for esthetic/ cosmetic reasons.
Movement of a Soft Contact Lens on the Surface of the Eyeball and behind the Eyelids. The Contact Lens moves with every gaze movement of the eyeball and also upon the frequent eye blinks. The amount of mechanical friction at the ocular surface is typically increased in contact lens wear, even when the tear film is sufficient.
The fact that Contact Lenses are sitting in the middle of the Ocular Surface has some pros and cons.
They certainly have some clear optical advantages ...
... but contact lenses still represent a ´foreign body´ for the Ocular Surface Tissues and Tear Film.
Even though contact lenses are typically ´swimming´ in the tear film it is still inevitable, that they are in mechanical contact with the ocular surface tissues.
A typical side effect of contact lenses therefore is the occurrence of increased frictional forces to the ocular surface tissues.
The fine structure of the surface epithelium may undergo a deterioration where it is exposed to the influence of a Contact Lens. Shown here is the change of the bulbar conjunctival epithelium in the excursion zone of a soft Contact Lens. The cubical surface cells with interspersed goblet cells for the production of water-adhesive mucins are replaced by a squamous epithelium without goblet cells in a process termed ´squamous metaplasia´.
Although fitting principles usually try to avoid too much physical ´touch´, contact lenses are still, inevitably, in contact with the ocular surface - just as their name suggests.
Contact lenses can thus have mechanical, physicochemical and chemical impacts on the Ocular Surface to varying degrees. Even though such contact lens impacts on the ocular surface may not necessarily be pathologic, they may still contribute to that is known as ´Contact Lens Discomfort´ (CLD). CLD refers to a vague irritative discomfort by sensing the presence of a contact lens on the eye and CLD was the topic and title of the 2013 TFOS report on such Contact Lens impacts on the Eye.
This concerns particularly the interference of the contact lens with the very sensitive central cornea and the similarly sensitive posterior lid border.
The conjunctival areas on the eyeball and on the back side of the lids are less sensitive, but are also in touch with the contact lens and are thus exposed to potential negative influences.
It is known for decades that chronic friction by a contact lens may negatively influence e.g. the fine structure of the conjunctival surface and thus reduce the wettability of the ocular surface. A typical side-effect in long-term contact lens wear is the potential development of Dry Eye symptoms of varying degrees.
It is shown that the structure of the bulbar conjunctiva changes in contact lens wear. This occurs in the zone where the margin of the contact lens is in touch with the surface and rubs over it upon every movement of the eye. The type of epithelium changes, termed as squamous metaplasia, and the number of goblet cells that produce the important mucus for the wetting of the surface, decrease in number. These alterations deteriorate the wetting of the Ocular Surface and promote the onset or worsening of Dry Eye Disease.
Apart from the fact that Contact Lenses can exert unwanted side effects on the ocular surface and tears Contact Lenses can also be used as a medical tool in selected cases.
The easiest case is probably when a soft Contact Lens is used as a clinical bandage lens to promote healing after surgery or in cases of recurrent corneal defects (erosions)
Several types of Speciality Contact Lenses exist that can be used as medical tools in selected medical conditions for patients who are in continuous clinical control.
This refers to ´Rigid´ Contact Lenses that can correct higher degrees of corneal shape distortion (as occurs in higher astigmatism and in keratoconus) where the visual acuity can not be sufficiently corrected by spectacles.
´Rigid´ Contact lenses can also be used for intended changes of the corneal shape, termed as ´Orthokeratology´ in order to avoid day time wear of spectacles - which certainly needs close clinical monitoring.
Even though contact lenses lead to alterations of the ocular surface fine structure with occurrence of dry eye symptoms ...
... Speciality Contact Lenses (Scleral Lenses) can be used as a medical tool in patients with severe Dry Eye Disease.
Scleral Contact Lenses provide a protecting translucent cover over the sensitive cornea and constitute a moist chamber that preserves the patient´s few own tears under the vault of the contact lens against evaporation. This can typically restore ocular surface healing and visual acuity.
Modern contact lens types can often reduce many of the potential negative impacts on the ocular surface by technical improvements - An issue that is still relevant is, however, the HYGIENE.
Insufficient Hygiene is a crucial factor in Contact Lens wear and results in a higher rate of ocular infections in contact lens wearers. Microbes can be introduced by the fingers of the wearer or from the use of tap water, that should be omitted. Certain types microbes also occur on the normal ocular surface. Microbes grow on the lenses and in the storage containers and form adhesive ´biofilms´ that protect them against cleaning and removal.
When basic rules of hygienic contact lens wear are not respected this can still result in dangerous ocular infections that may endanger vision.
Even with application of the most advanced medical therapy, a severe contact lens related corneal infection may eventually and tragically lead to a loss of the eye.
Bacteria are typically introduced through the handling of the contact lens by the wearer and/or by use of contaminated tap water. Bacteria accumulate in the contact lens containers or in difficult to remove deposits on the contact lens itself.
The occurrence of infection is further promoted by the inevitable occurrence of tissue microtrauma of different kind in contact lens wear. This provides a route of entry through the normally almost impenetrable ocular surface barrier.
Particularly inexperienced Contact Lens wearers are at risk for serious ocular infections. Furthermore patient groups with a reduced level of immune defense such as children and elderly people are particularly susceptible to ocular surface infections.
The increased use of daily disposable contact lenses contributes to a decrease in ocular infections. because the critical steps of cleaning and storage of a worn lens become obsolete.

Choose your CHAPTER of Interest - or simply read along ... which may be most instructive






The OCULAR SURFACE must be constantly moist to provide its health and thus perfect vision.
The OCULAR SURFACE is the moist mucosal tissue at the anterior side of the eye ball. Apart from the readily visible Cornea and Conjunctiva that are bathed in the tears it consists of the Lacrimal Gland for production and of the Lacrimal Drainage System for disposal of the ´used´ tear fluid.
The CONJUNCTIVA is a maintenance organ for the cornea that contributes to the health of the cornea. It covers the front side of the eye ball and the back side of the eye lids and thus forms the conjunctival sac that is open to the outside only at the palpebral fissure where the tissue is covered by a film of tears - the tear film. (The width of the conjunctival sac and tear film are greatly exaggerated in the schematic drawing for didactic reasons - normally the eye lids basically touch the globe and transform the ´real´ conjunctival sac into a mere moist slit between the eye lids and the eye ball and the tear film is very thin.).
The Ocular Surface is a moist mucosal tissue to keep the Cornea transparent.
It must be kept constantly MOIST – everywhere and every time – to remain healthy and intact and the Ocular Surface is thus constantly bathed in the tear fluid.
The vehicle for moisture are the TEARS that are produced by the ocular glands and disposed by the lacrimal drainage system into the nose.
The continuous Turnover of Tears at the Ocular Surface goes (1) from their main production in the lacrimal gland over (2) the readily visible cornea and conjunctiva that they must constantly bathe into (3) the lacrimal drainage system that drains the tears into the nose.
The Tear FLUID, usually simply termed as ´TEARS´ is produced/ secreted by the Glands of the Ocular Surface.
After their ´usage´ at the Ocular Surface, which refers to the bathing of the cornea and conjunctiva ...
... the tears are discharged from the bulbar surface into the lacrimal drainage system towards the nose.
The continuous production of new tear tears and their flow over the ocular surface is therefore of utmost importance for the health and clarity of the CORNEA and thus for intact VISION.
Also, the regulated disposal of ´used tears´ from the ocular surface is very important because there is very little space on the ocular surface for fluid.
Actually not even one drop of extra fluid, e.g. of eye drops, can typically be accommodated and thus most of it typically flows away over the lid margin
In contrast to a real DRY Eye, with a definite lack of tears, the increased production of tears as seen in an irritated ´Watery´ Eye ... or, a decreased disposal of tears from the ocular surface, as seen in an abnormal eyelid shape termed as ´ectropion´ can also lead to problems.
Both of these conditions with ´too many tears´ at the ocular surface typically lead to a (continuous) dripping of tears over the lid margin, that is termed ´epiphora´ by the clinician.
So ... we can see that the ocular surface is not too different from our experience in daily life - too much can be equally tiresome as too little.
Constant moisture of the cornea and conjunctiva in the opened palpebral fissure is achieved by covering them with a layer of tear fluid – The TEAR FILM.
This is thin and homogeneous enough not to impair vision and at the same time sufficiently stable to avoid desiccation of the tissue at the air atmosphere.
The Tear FILM has three layers constituted by the products of different glands. Mucins from single goblet cells (GC) in the conjunctiva make the surface wettable by the Water from the Lacrimal Gland. Oil from the Meibomian glands inside the eye lids forms the surface - it retards evaporation of the tear water and provides stability of the tear film.
A glimpse into the TEAR FILM. The main phase of the Tear Film overlying the transparent cornea is composed of the aqueous fluid from the lacrimal gland. Below are the numerous finger-like protrusions of the surface cells. Their cell bound and and loose secreted mucins (pink filaments) constitute the basal mucin layer that binds the tear water to the ocular cell surface. Mucins mix with the water and together they form a water-mucin gel. The surface of the Tear Film is covered by a very narrow oil layer from the-lipids of the Meibomian glands. The lipid layer has the same thickness and coloring as an oil film on a puddle of water. A main function of the oil layer is to retard the evaporation of the aqueous main phase of the tears. Consequently a lipid deficiency due to a dysfunction of the Meibomian glands is presently reported as the main causative factor for Dry Eye Disease.
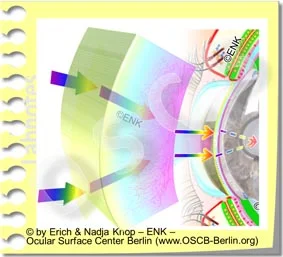
This schematic animated diagram illustrates the principal eye lid function of tear spreading - actual tear drops occur in the palpebral fissure only during increased tear secretion.
The wiping movement of the upper eyelid during the blink spreads the tears into the thin and homogeneous Tear FILM.
Of particular importance at the eyelid margin is the posterior lid border because this is the structure that distributes the tears into a very thin film of tears. The posterior lid border acts similar to the wiper blade at the windscreen of car. It is therefore termed the lid wiper.
This blink movement of the Eyelids is not only necessary for keeping the moisture of the tissue in the palpebral fissure ...
The wiping movement of the upper eyelid during the blink spreads the tears into the thin and homogeneous Tear FILM.
This blink movement of the Eyelids is not only necessary for keeping the moisture of the tissue in the palpebral fissure ...
... but, at the same time, the tear film is the main surface for refraction of the light to provide perfect vision.
Another function of the blink is that the force of the lid muscle expresses some oil from Meibomian oil glands inside the Eyelids.
A lack of blinking therefore leads to a lack of oil on the tear film and to its instability.
In conclusion, the necessary prerequisites for a stable Tear Film and thus for ocular surface health and visual acuity are Secretion of tear fluid by the glands and the Formation of the tear film by the blinking action of the eyelids …
... consequently an alteration of Gland function and/ or of Eyelid function may lead to a Dry Eye condition - if this occurs chronically it may result in Dry Eye Disease.
In addition to spreading the Tear Film from the tear fluid, the eyelid action during blinking also contributes to the drainage of the used tear fluid via the lacrimal drainage system into the nose.
The healthy Ocular Surface provides the clear window of the eye to see the light from the environment.
Without a healthy ocular surface all later steps of the vision process are meaningless.
DRY EYE DISEASE is an impairment of permanent moisture of the Ocular Surface with subsequent Destruction of the Tissue and a Reduction of Visual Acuity.
Dry Eye Disease is often termed as ´KeratoConjunctivitis Sicca´ (KCS) or simply known as ´Dry Eyes´, Burning Eyes, Itchy Eyes, Heavy Eye Lids, Tired Eyes ... and many other colloquial expressions that refer in one or the other way to ocular irritation.
Dry Eye Disease is a complex dysregulation of the functional anatomy of the ocular surface that impairs the permanent moisture and the integrity of the tissue and thus its health and the intact vision.
It typically goes along with signs and symptoms of ocular dryness, ocular irritation, tissue destruction and pain as well as with visual impairment, mainly in the sense of fluctuating visual acuity. and blurred vision.
Basic CAUSATIVE FACTORS for the pathology are:
The alterations in the function of the ocular glands and/ or of the blinking mechanism lead to INSTABILITY of the Tear FILM and thus to impairment of permanent ocular surface wetting. Insufficient wetting then results in DAMAGE of the Ocular Surface Tissue !
The basic causative factors of insufficient secretion and/or insufficient tear film formation ...
... lead to the primary pathologies of Tear Film instability and subsequent Drying and Damage of the Tissue
These two pathologies explain the typically SYMPTOMS in Dry Eye Disease::
e.g. intermittent blurred vision that comes and goes and becomes better upon enforced blinking - which is good evidence that the symptoms indeed derive from a Dry Eye condition.
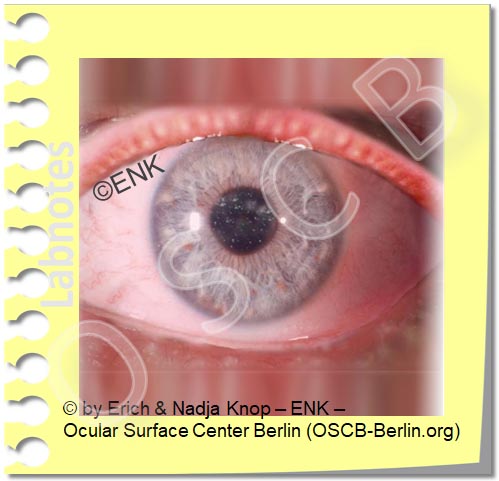
A moderate DRY EYE typically shows only mild redness of the Conjunctiva and Lid Margins that may indicate an inflammatory condition as described by the term ´Keratoconjunctivitis sicca´. The orifices of the Meibomian oil glands are often obstructed by visible or invisible inspissated secretum (which represents the most frequent primary cause of Dry Eye Disease). The tear volume is low due to water evaporation and the tissue of the Ocular Surface epithelium has many small defects, that occur as small spots in vital staining with a green stain (fluorescein) observed in blue light.
The lack of sufficient tear fluid or a lack of a sufficiently stable Tear Film, that is often caused by a Dysfunction of the Meibomian Glands (MGD), results in the pathological SIGNS of the Dry Eye Disease.
The typical signs of Dry Eye Disease are important to known and are useful for the Diagnosis:
initially, occasional episodes of increased tear flow and watery eyes can alternate with eye dryness
In Dry EYE DISEASE there is often a Disparity between subjective Symptoms of the Patient and the objective clinical Signs points to some considerations on the neurobiology.
The processing of signals from the Ocular Surface is complex and is influenced on different levels of the nervous system. Therefore, the outcome depends on many variables and may very well be different in different individuals. This fits well with the observations from our daily lives, that different people tend to have different ´nerve costumes´ and may react differently to the same stimuli.
Another issue is, that there is a principal difference between a ´perception´ e.g. of touch in a peripheral organ, such as the cornea, and the allocations that subcortical centers add to it in order to produce something that we call pain.
PAIN is not a mere perception but is basically more of a feeling, i.e. a construction of the brain, because it contains an emotional aspect that the brain allocates to an incoming afferent impulse from the periphery.
The emotional aspect that the brain allocates to the stimulus is based on very individual things like previous experiences, recent emotions, or future expectations ... in order to name just a few factors. Therefore the actual feeling that is generated in the brain can vary to a large degree in different individuals. This may point to a neuro-biological explanation of the disparity of signs and symptoms in Dry Eye Disease.
However, for the respective individual, the two different neurobiological authorities of "perception´ and of ´pain´ are not always clearly discernible ... and it is not always clear which of the authorities is more ´real´ and thus trustworthy.
Pain has the biological sense to alert us in order to avoid dangers that may threaten our health or our life. Under certain conditions when a pain becomes chronic and when it leads to a damage of the nervous system itself, it can develop into a chronic PAIN SYNDROME. Pain has then lost its biological function and becomes a disease of its own. In such cases where chronic pain persists without an identifiable tissue damage it may be useful to seek the help of a pain specialist.
The subjective emotional rating of a sensation may very well dominate over the pure perception ... or reverse. In some cases intense subjective symptoms are causing a severe suffering of the patient whereas the clinical investigation may only observe few minor manifest alterations or even now pathology - this may probably point to a potential chronic pain syndrome.
On the other hand there may be a patient who in fact has severe objective alterations of the normal structure and function but does not suffer from any severe symptoms or may probably have no symptoms at all. Such a patient may then have only a limited interest in therapeutic interventions even though these may be very advisable from a clinical perspective.
Psychosomatic Influence on a disease process and on its self-perception by the patient are an established and well recognized part of medicine for a long term. Apart from e.g. back pain, cardiovaculatory dysfunction, and intestinal dysfunction, a psychosomatic component can play an important role also in Dry Eye Disease, as confirmed by many studies. When the disease becomes the main concern in daily life this may suggest that it could be useful to seek the help of psychosomatics.
An impairment of positive factors and the occurrence of negative factors both decreases the normal function of the tissue and thus increase the likeliness and severity of a potential Dry Eye Disease.
The complex dysregulation of the functional anatomy of the ocular surface in Dry Eye Disease with a deficiency of the basic functional complexes for permanent moisture is influenced by different factors:
Failure of mainly the Nervous System, Endocrine Hormonal System, and the Immune System deteriorates the function of the Ocular Surface. Age and female Sex, related to a predominating estrogen action with relative lack of androgens, appear as the main predisposing factors for a higher risk of Dry Eye Disease
Negative external influence factors represent RISK factors for disease. They influence the tears on the surface and can override the normal functional capacity. They mainly occur in desiccating environments, contact lens wear, visual tasks with low blinking frequency. Many occur combined in typical office work environments and may lead to a Dry Eye Condition termed "Office Eye".
Negative internal influence Factors represent RISK factors of the onset of disease. They act on the tissues that produce the tear fluid and can deteriorate the normal function. These are e.g. chronic diseases, chronic medication, age, sex, nutrition or hydration etc.
The complex pathologic events in Dry Eye Disease tend to influence each other negatively and thus form self enforcing VICIOUS CIRCLES of Disease Progression.
This does often lead to a worsening of disease without a timely diagnosis and an effective therapy.
Inflammation is an important mechanism for worsening of Dry Eye Disease.
Inflammation is a basic protective mechanism of cells and tissues against wounding and destruction, as typically occurs in Dry Eye Disease due to tear film instability and increased friction. Inflammation initiates destructive mechanism in order to overcome the ´destructor´ and is later followed by tissue repair.
When inflammation becomes chronic, however, it transforms into a negative and destructive process because the initial destruction can not be followed by a sufficient repair.
In chronic diseases like Dry Eye Disease, the chronic tissue wounding may lead to a chronic inflammation that drives some vicious circles and can thus greatly enhance the disease process.
Dry Eye Therapy to interrupt the vicious circles in Dry Eye Disease may then include an anti-inflammatory therapy for a limited time in addition to a sufficient Tear Supplementation and Eyelid Therapy .
For more detailed information on THERAPY in Dry Eye Disease please see the Full Length English Language Pages of the OSCB
Most of us have probably already had an occasional sensation of a “dry” eye, e.g. when we are exposed to an unusually dry and desiccating environment, characterized by Low humidity, hot temperatures, high wind speeds and/ or by Low blinking frequency due to intensely concentrated visual tasks as e.g. in screen work
Such a “dry” eye is is typically a short-lived condition that disappears as soon as we become aware of it and remove the described desiccating stimulus.
Only when the feeling of “Dryness” remains constantly and cannot be removed or sufficiently improved by avoiding desiccating environmental stimuli and/or by improving blinking
… then the conditions becomes chronic and an occasional “Dry” Eye may develop into Dry Eye DISEASE.
This is typically related to an increase in duration and intensity of symptoms and by increasing severity of clinical findings/ signs due to increasing alteration and wounding of the ocular surface tissue
Several Different and Interacting self-enforcing VICIOUS CIRCLES of disease aggravation and worsening occur in chronic Dry Eye Disease and can lead to the full blown clinical picture with a progressive tissue destruction and a loss of function of the ocular surface.





