

Content of this page:
Modern Scleral Lenses are a high tech medical tool for severe ocular surface disease
Scleral Contact Lenses have a (relatively) short adaptation time because they cause minimal interaction of the lens margin with the lid border
Specific construction principles of Scleral lenses allow preservation of the ocular surface. Sclerals contact lenses form a protective aqueous vault over the cornea.
Corneal ectasia / Keratoconus is a prime indication for Scleral Contact Lenses to restore vision and to adjourn surgery
Scleral contact lenses can restore the Ocular Surface Functional Unit
Severe Dry Eye Disease is an important indication for Scleral Lenses
Modern Scleral Lenses are a high tech medical tool for severe ocular surface disease
Modern scleral lenses have emerged as a new and ever more exciting medical tool for the dedicated ocular surface specialist in recent years. This represents a rejuvenation of the scleral lens concept after its decline during the last century that had occured due to complicated lens fitting and inappropriate lens materials with consequent long adaption times of the wearer.
New fields of application and medical indication have emerged for scleral contact lenses with exciting treatment results have meanwhile occurred. This is due to the advent of new lens materials and, more so, of computer assisted lens designs, automated measurement of the ocular surface topography, lens manufacturing on demand based on this data, and high-tech lens material properties. These technological improvements have led to a renaissance of the Scleral Contact Lens.
Scleral Contact Lenses have a (relatively) short adaptation time because they cause minimal interaction of the lens margin with the lid border
The described technological advancements have distinctly improved the fitting as well as the wearing of scleral lenses with high oxygen permeability. To some surprise, patients often consider a large scleral lens as the type of contact lens that is causing the least ocular irritation on the ocular surface as compared to other contact lens types of smaller sizes, in particular RGP lenses.
This may in part be due to the permanent location of the margin of the large scleral lenses underneath both the upper and the lower eye lid. In the large scleral lenses the posterior lid margin, that has an enormously high sensitivity, does not have to hit the lens margin during every single one of the frequent blink movements. This applies mainly to the upper eye lid margin that must glide over the contact lens margin but, during a blink. A corneal or smaller corneoscleral contact lens also touches the lower lid margin before it re-centers on the cornea after a blink.
Specific construction principles of Scleral lenses allow preservation of the ocular surface

Scleral lenses have some typical construction characteristics, that make them different from, and in many ways superior to, other lens types.
Sclerals typically do not touch the cornea at all because they rest on the peri-limbal sclera whereas the cornea is constantly bathed in a tear lake underneath the center of the lens.
The term ´scleral´ lens is actually not perfectly correct because sclerals are in fact resting on the bulbar conjunctiva that is overlying the sclera. So, the weight of the lens is mainly exerted onto the conjunctiva and not the sclera.
Scleral contact lenses form a protective aqueous vault over the cornea
The advantage of not touching the cornea is achieved by a special lens geometry with three zones that have a different curvature:
The central zone is the optical zone, also called vault because is covers the cornea like a dome without touching it. The area under the dome is filled with the patient’s own tears.
The peripheral landing zone / haptic is less steep because the sclera of the eye ball has a larger curvature compared to the cornea.
In the intermediate zone, typically overlying the corneal limbus, both curvatures transform into each other.
Corneal ectasia / Keratoconus is a prime indication for Scleral Contact Lenses to restore vision and to adjourn surgery
Keratoconus is a prime case for the use of Scleral Contact Lenses for at least two reasons.
The irregular protrusion of the cornea leads to higher order disturbance of refraction and distinct loss of visual acuity that can for visual rehabilitation only be corrected by providing a new smooth regular outer surface. The new regular optical surface as provided here by the outer surface of the scleral lens that is internally filled by the optical medium of the tears.
This protrusion of the cornea is typically associated with a distinct thinning of the tissue that is prone to rupture of the cornea and thus opening of the eye. This is extremely dangerous not only because of high risk of infection of the whole eye but also because of the loss of internal pressure of the eye ball with a number of deleterious downstream effects.
Scleral contact lenses can restore the Ocular Surface Functional Unit
The covering of the complete cornea including the peripheral limbal stem cell region in a permanent bath of the patient´s own tears underneath the vault of the scleral lens restores important aspects of the ocular surface functional unit (for details please see the Section on Ocular Surface). The cornea remains moist and is regulated by the nutritive and regulatory factors in the tears whereas mechanical friction forces are largely absent because the cornea is shielded by the dome (for details please see the section on Cornea).
Chronic irritation can thus calm down and the ongoing unsuccessful repair mechanisms, that are a part of chronic inflammatory responses, remain undisturbed. Constant immersion of the cornea in the tears allows an improvement and often healing of chronic pathological processes at the ocular surface such as e.g. recurrent corneal erosions and ulcerations. Surprising improvements are also reported in cases of corneal opacity and scars.
Severe Dry Eye Disease is an important indication for Scleral Lenses
Severe cases of dry eye disease are therefore another important application of scleral lenses. This may be of some surprise because a deficiency in tears us typically considered as a limiting factor for contact lens wear or may even represent a contra-indication when the Dry Eye is severe.
This applies, however, only to the use of conventional ´cosmetic´ contact lenses, such as soft corneoscleral lenses or the small rigid gas permeable lenses - as described in the ´BLINK´and OVERVIEW´ pages of this chapter. These ´conventional´ contact lenses are ´swimming´ in the pre-ocular tear film and thus require a substantial tears volume.
Scleral contact lenses in contrast are kind of ´sealing´ the available tears, like a lid on a pot, and thereby Sclerals are ´saving´ and accumulating the available limited tear volume.
Scleral contact lenses therefore provide a restoration of the ocular surface unit that allows for an amelioration of the chronic irritation impacts of friction and hyper-osmolarity in Dry Eye Disease. This leads to a consequent decrease of the downstream inflammatory reactions and of the resultant self-perpetuating vicious circles.
Under scleral contact lenses the ocular surface tissue can heal and regenerate without disturbance by the adverse effects of ocular dryness. Sclerals are therefore an effective tool to interrupt the vicious circles of disease amplification and propagation.
Conventional contact lenses - here a small ´rigid´ gas permeable (RGP) lens - swim in the tear film and need copious tears ... which is a clear disadvantage in Dry Eye Disease and make ´conventional´ contact lenses unsuitable in this condition.
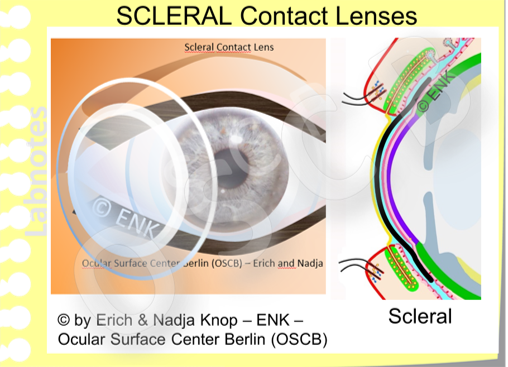
A SCLERAL CONTACT LENS in contrast can shield the whole cornea including the limbal epithelial stem cell zone against external influences. Even during blinking it remains relatively stable and provides a constant bath of the cornea within the tear fluid - as explained above.