
Deeper Insight - How can we TREAT Dry Eye ? ...
THERAPY 4 - MGD Therapy - PHYSICAL Therapy
Eye Lid WARMING
Meibomian GLAND EXPRESSION
AUTOMATED WARMING & Gland EXPRESSION
Lid HYGIENE & Lid SCRUBS
... => Tear SUPPLEMENTATION is covered in a separate Chapter
Meibomian Gland Dysfunction (MGD) appears as the main reason for Dry Eye Disease

The TFOS-MGD Workshop Report in 2011 has led to a change of paradigms in the view on the pathophysiology of Dry Eye. There is evidence to suggest that in fact not a primary aqueous deficiency but instead a primary lack of lipids from the Meibomian Glands, due to Meibomian Glands Dysfunction (MGD), appears in fact to be the main primary causative factor for the onset of Dry Eye Disease. This occurs in about four fifths of patients as similarly reported in several studies.

This has virtually opened the eyes for therapy options that are directed to New THERAPEUTIC TARGETS

The main pathogenetic factors for obstructive Meibomian Gland Dysfunction are an inspissation of the lipid secretum due to increase melting point and a hyperkeratinization of the ductal system and lid margin.
The CORE MECHANISM of Obstructive MGD is based on 2 Pathogenic Factors
The typical pathogenetic factors that lead to obstructive Meibomian Gland Dysfunction (MGD) are
- a HYPER-KERATINIZATION of the ductal system together
- with INCREASED VISCOSITY of the Meibomian Secretum (termed Meibum)
They constitute the CORE MECHANISM together with the resulting
- Gland OBSTRUCTION
THERAPEUTICAL TARGETS are:

(1) the LIPID PHASE of the tears
- LIPID DEFICIENCY/ LACK on the tear film:
- => evaporation of aqueous tears / Evaporative Dry Eye Disease
- => aqueous tear deficiency only secondary
- THERAPY => LIPID SUPPLEMENTATION
(2) the MEIBOMIAN GLANDS and their Content
- Lipid Stasis, Increased Pressure inside the gland
- (2 A) Gland, TISSUE PRESSURE ATROPHY
- THERAPY
- => PHYSICAL THERAPY
- THERAPY
- (2 B) Gland, LIPID SECRETUM INSPISSATION inside
The Pathology inside the gland can be severe
Obstruction blocks the outflow of Meibomian oil onto the lid margin and leads to :
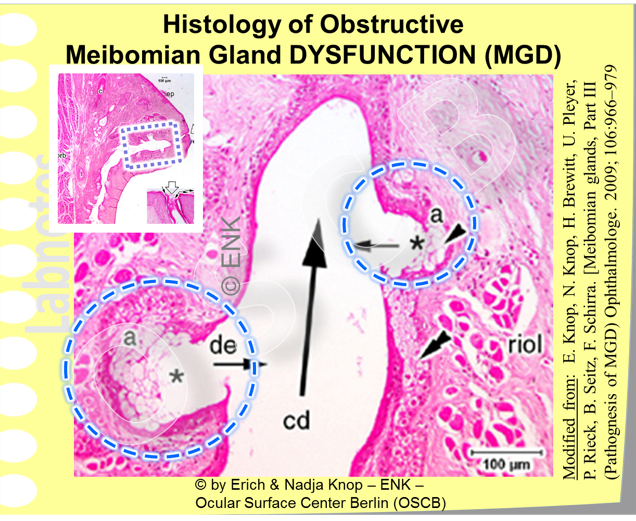
Increased pressure inside the Meibomian glands leads to a PRESSURE ATROPHY with (1) Dilatation of the ductal system, (2) Destruction and Rarefication of the secretory Meibocytes in the Acini and (3) Destruction of the Acini and integration or acinar remnants into the ductal wall. (An overview of a gland in the left top corner shows the area where the higher magnifications of the main image comes from - histological photomicrographs in H&E stain)
Increased pressure inside the glands... with downstream potential destruction of the gland tissue by a PRESSURE ATROPHY with:
- (1) destruction of the ductal system by dilatation
- (2) destruction of the secretory cells (Meibocytes) in the acini which can include
- (3) destruction of the acini and integration of remnants into the ductal wall
MGD Therapy: ... offers the UNIQUE CHANCE for a causative or semi-causative approach in Dry Eye Disease by Physical Therapy
Physical Therapy in MGD

- WARMING of obstructed glands
- to re-liquify the secretum that is inspissated due to the occurrence of aberrant lipid species with increased melting point
- EXPRESSION of obstructed glands
- LID HYGIENE
- to remove debris from lipid depositions
- and epithelial squames together with
- opportunistic microbes
The RATIONALE behind Meibomian GLAND EXPRESSION
... is to remove the obstruction and release the stasis ... in order to relieve the glands and those secretory Meibocytes that are (still) intact from the internal pressure to give them a chance to heal and re-constitute functional gland tissue as far as possible.
Meanwhile there is even an automated simultaneous eye lid warming and expression device available for the clinician that can effectively treat obstructed glands. Physical gland therapy can in selected cases be added by mild anti-inflammatory or antibiotic or by a combined therapy.

Eye LID WARMING - A Pre-Treatment before gland expression
The RATIONALE behind Eye lid warming is:
- the concept that the increased viscosity of the Meibomian Lipids inside the gland results from the occurrence of lipids with an increased melting point and from
- the observation by TIFFANY, BRON and colleagues, that the melting point of normal Meibomian lipids is already relatively high and only slightly below the temperature inside the eye lids - so that any elevation will likely result in lipid inspissation
- the observation of BLACKIE and KORB that the physical expression of inspissated Meibum without prior warming can be quite painful ... so that only few individuals can tolerate it
The temperature for lid warming must be adequate
... but the immediate question is: "WHAT is adequate temperature ?"
"Adequate" means ... WARM enough to re-liquifiy the inspissated lipids ... but NOT too HOT- in order to prevent burning of the tissue of the eye lids and of the cornea.
Since the coagulation of protein is typically thought to start over 42°C for liquid egg-white, even though higher temperatures are reported for tissues, the temperature should not much exceed 42°C. at the inner side of the eye lid.
According to investigations by BLACKIE and colleagues who used
- (1) moist compresses
- (2) at 45°C with
- (3) replacement every two minutes,

- it requires 4 to 6 minutes to reach a maximum outer lower lid temperature of 43°C ... and
- it takes even 30min (which would include to replace the warm compress 15 times for a new one !) to reach a maximum inner lower lid temperature of about 40,5°C.
From these investigations it can be concluded that:
- when the temperature of moist warm compresses is limited to 45°C, there is apparently no danger of burning the tissue
- BUT ... the warming of the eye lids is labor-intensive and takes time and effort.
There are SEVERAL DEVICES for EYE LID WARMING
Several commercial devices have been developed in order to make eye lid warming before manual expression less labor-intensive ... at least by making the frequent replacements of warm compresses unnecessary. There are mainly two approaches:
EYE LID COVERS / GEL MASKS - they are very popular

- in the form of glasses that cover both lids and
- that are typically filled with some kind of gel
- that typically require heating in a warm water bath or in a microwave oven
- an additional advantage is that gel masks can also be used cold in order to get relief for inflamed eyes, e.g in ocular allergy
- ... these Gel Masks are definitely helpful and make life easier and they are inexpensive - still the questions occur
- how exact the temperature is controlled by the patient - which is certainly difficult
- how long the temperature is kept before also such a mask must be replaced
AUTOMATICALLY HEATED GOOGLES
AUTOMATIC GOOGLES are a great advancement and make Physical MGD Therapy much easier because they control the temperature and do not need replacements. The water source is typically some kind of hydrophilic soaking material that stays moist for one complete use-cycle.

- automated googles look indeed like googles for swimming
- they fit tight to the head because they typically contain moisture of some kind
- they are electrically warmed which allows to control the temperature exactly
- they don´t need to be replaced because the temperature remains constant

The BLEPHASTEAM Googles for automated application of exactly dosed heat together with moisture is probably the most well known type of MGD Googles Image: Courtesy of THEA Pharma..
The googles are more user-friendly and probably particularly advisable to the elderly - who are at the same time the typical age group that appears most affected by MGD at present.
A new google generation is supposed to resemble more a stylish smartphone with attached power pack and eye-glasses - probably the right Meibomian Gland Rejuvenation for the 24/7 professional electronic computer screen user generation with a notorious lack of blinking and a potential risk for Meibomian Gland Dysfunction. This population typically suffers from who suffer from the more modern condition of ´office eye´
Warming & Heating Googles are certainly more expensive because of the applied technology - but they are less expensive than even a cheap smartphone - so this should be no major hurdle when ocular health is concerned.
EXPRESSION of Meibomian GLAND remains to be done after warming ... and can be AMBITIOUS

Manual Meibomian Gland EXPRESSION with the own fingers is possible only to a limited extent and mainly for the lower eye lids as shown here. Expression between thumb and index finger is most effective in the middle of the lid, whereas the nasal and temporal regions are less accessible. Only small amounts of inspissated secretum are expressed here from two orifices in about the middle along the lid.
Expression of the Meibomian glands is much easier after lid warming when the lipids inside the glands are re-liquefied.
Technically it is, however, ambitious to express:
- at least one´s own eye lids and
- to do it manually with the fingers
- please see the image to the right
- particularly difficult is expression of the upper eyelids
ONE IMPORTANT Reason for some inconvenience is ... that the Meibomian Glands must NEVER be expressed from the outside AGAINST THE EYE BALL (!) ... because this can potentially cause severe wounding to several internal tissues, most likely retinal detachment is a not too theoretical danger, at least in predisposed individuals !
In the clinicians PRACTICE, with appropriate instruments, expression of the eyelids is much easier (please see clinical photos below).

- Typically an Eye Lid PLATE or a Mastrota Paddle is used, that is held behind the back, i.e. the internal, side of the lids on the conjunctival surface
- The pressure is then typically exerted with a finger or a sponge onto the lid skin over the Meibomian Glands and against the lid plate
- Alternatively, a sufficiently stiff Q-Tip-like sponge on a stick or only a sponge is held on the posterior side.
By these techniques an effective expression of the Meibomian glands is usually possible. Inspissated secretum, but previously re-liquified, is typically expressed until the glands are completely emptied.
Expression-FORCEPS
Different types of Forceps have recently been developed in order to simplify the expression of the Meibomian Glands.
This appears as a favorable innovation that may particularly make the gland expression easier for the MGD patient himself - although a treatment in the practice of the clinician is certainAly more advisable in order to avoid any risk of wounding.
AUTOMATED Lid WARMING and Meibomian Gland EXPRESSION
The RATIONALE for AUTOMATED and COMBINED Eye Lid WARMING together with subsequent EXPRESSION of the Meibomian Glands comes from the observations that were made during clinical studies, that:
- Gland EXPRESSION tends to be painful without prior lid warming
- Efficiency of Expression depends on the particular experience of the investigator and on the degree of obstruction and lipid inspissation
- but Eye Lid WARMING
- is time consuming and potentially inefficient when the applied hot pads are not frequently changed
- since it is recommended to repeat the manual expression regularly - it may be assumed that this is not very effective and at least the glands are not completely emptied
Therefore the clinician who had once discovered the condition of obstructive MGD (Prof. Donald KORB from Boston, MA), and who has since then treated so many patients with MGD, has developed an automated technique that is performed by a custom-tailored and computer regulated device.
A principle technical advantage comes from insight into the Anatomy of the eye lids:

- the Meibomian Glands are located in the posterior half of the eye lid, right underneath the conjunctiva
- the manual warming, however can, for technical reasons and for safety, only be applied from the outside through the skin and lid muscles
- this makes ii ineffective
- explains why it takes so much time and effort
=> this has lead to a Revolutionary Idea:
- the heating is directed to the BACK SIDE of the lids and
- thus directly to the Meibomian glands
- applied by an automated computerized device
- that protects at the same time the sensitive cornea
This device has proven to have many advantages compared to even an optimally experienced manual therapy:

The most innovative and effective treatment for obstructive Meibomian Gland Dysfunction is presently an automated simultaneous lid warming and gland expression procedure. This is achieved by the LIPIFLOW device that was built according to the ideas of Prof. Donald Korb from Boston, MA, who is a one of the most experienced clinician for Meibomian Gland Dysfunction. (Images: Courtesy of TearScience Inc.)
- it keeps the optimal temperature level for the whole procedure
- it is more effective than a manual procedure
- it is quicker than a manual procedure because it takes only 10 minutes for one eye
- it is completely safe and in fact appears to feel as a wellness procedure for the lids as patients report afterwards
- it apparently has an amazing long-term effect
Several peer-reviewed reports from scientific studies have observed an amazing long-term effect after a single Lipiflow procedure. It is reported, that an improvement of objective clinical signs lasts over one year and improvement of subjective symptoms lasts even longer than two years.
From these results it may conceivably be concluded that an effective removal of gland obstruction and respective internal pressure from stasis of accumulated lipids may indeed lead to a re-vitalization of remaining secretory cells.
LID HYGIENE
LID HYGIENE is typically done with some kind of disposable pad similar to those that are used for removing make-up. In addition some kind of liquid is applied from clean water to special lipid solutions - the use of detergents, however would likely disturb the tear film lipid layer. The more vigorous the hygiene becomes, the more it transforms into a lid SCRUB which needs a certain carefulness in order to avoid wounding.
Lid Hygiene is a suitable final step after gland expression in order to remove debris from the lid margin that may be inflammatory or otherwise contaminated.
Lid Margin Debris can typically consist of:
- inspissated altered lipids
- including irritant lipid species such as free fatty acids
- epithelial hyper-keratinized material
- dust and environmental antigens
Soaps or detergent solutions may negatively affect lipids in the tear film lipid layer and are thus not very advisable.
Clean warm water or physiological saline solution appear better suited - lipid solutions are frequently used comparable to removing make-up together with a suitable pad to clean the lid margin.
Lid MASSAGE and/or Lid SCRUBS
Often the Lid "HYGIENE" is combined with a gentle massage of the eye lids in order to try to empty glands that are blocked to a minor degree. This works often better when by a gentle lid scrubs lid margin debris, that may be potentially block Meibomian orifices, is already removed.
A lid "SCRUB" is more vigorous than just a gently cleaning ... but there is certainly no concrete border line from one to the other. The more vigorous the lid ´scrub´ is performed, at least if this is not done by a well-educated specialist, the higher the risk for any kind of wounding may be estimated.
Just repeated careful cleaning of the lid margin twice a day typically has a positive effect on gritty lid margins with obstructed Meibomian glands ... and subsequently on the dry eye condition.
There are several commercial sets available for performing lid hygiene. They definitely have the advantage, that everything is right at hands in a suitable and handy way.