
Deeper INSIGHT ...
... into the function of the Ocular Surface and the development of Dry Eye Disease

Choose your CHAPTER of Interest - or simply read along ... which may be most instructive




The Ocular Surface
The OCULAR SURFACE must be constantly moist to provide its health and thus perfect vision.
What IS the Ocular Surface ?
=> The moist tissue at the anterior side of the eye ball !
The OCULAR SURFACE is the moist mucosal tissue at the anterior side of the eye ball. Apart from the readily visible Cornea and Conjunctiva that are bathed in the tears it consists of the Lacrimal Gland for production and of the Lacrimal Drainage System for disposal of the ´used´ tear fluid.
The CONJUNCTIVA is a maintenance organ for the cornea that contributes to the health of the cornea. It covers the front side of the eye ball and the back side of the eye lids and thus forms the conjunctival sac that is open to the outside only at the palpebral fissure where the tissue is covered by a film of tears - the tear film. (The width of the conjunctival sac and tear film are greatly exaggerated in the schematic drawing for didactic reasons - normally the eye lids basically touch the globe and transform the ´real´ conjunctival sac into a mere moist slit between the eye lids and the eye ball and the tear film is very thin.).
Why is the Ocular Surface Moist ?
=> To preserve its health and integrity !
Only a moist cornea can stay transparent
The Ocular Surface is a moist mucosal tissue to keep the Cornea transparent.
It must be kept constantly MOIST – everywhere and every time – to remain healthy and intact and the Ocular Surface is thus constantly bathed in the tear fluid.
The vehicle for moisture are the TEARS that are produced by the ocular glands and disposed by the lacrimal drainage system into the nose.
The continuous Turnover of Tears at the Ocular Surface goes (1) from their main production in the lacrimal gland over (2) the readily visible cornea and conjunctiva that they must constantly bathe into (3) the lacrimal drainage system that drains the tears into the nose.
TEARS are the Essence and Medium of Moisture at the Ocular Surface
The Tear FLUID, usually simply termed as ´TEARS´ is produced/ secreted by the Glands of the Ocular Surface.
After their ´usage´ at the Ocular Surface, which refers to the bathing of the cornea and conjunctiva ...
... the tears are discharged from the bulbar surface into the lacrimal drainage system towards the nose.
The continuous production of new tear tears and their flow over the ocular surface is therefore of utmost importance for the health and clarity of the CORNEA and thus for intact VISION.
Also, the regulated disposal of ´used tears´ from the ocular surface is very important because there is very little space on the ocular surface for fluid.
Actually not even one drop of extra fluid, e.g. of eye drops, can typically be accommodated and thus most of it typically flows away over the lid margin
In contrast to a real DRY Eye, with a definite lack of tears, the increased production of tears as seen in an irritated ´Watery´ Eye ... or, a decreased disposal of tears from the ocular surface, as seen in an abnormal eyelid shape termed as ´ectropion´ can also lead to problems.
Both of these conditions with ´too many tears´ at the ocular surface typically lead to a (continuous) dripping of tears over the lid margin, that is termed ´epiphora´ by the clinician.
So ... we can see that the ocular surface is not too different from our experience in daily life - too much can be equally tiresome as too little.
What is the Tear FILM ... and what is it good for ?
=> it is a fluid film with a certain layered structure
=> It provides Moisture and Vision !
Constant moisture of the cornea and conjunctiva in the opened palpebral fissure is achieved by covering them with a layer of tear fluid – The TEAR FILM.
This is thin and homogeneous enough not to impair vision and at the same time sufficiently stable to avoid desiccation of the tissue at the air atmosphere.
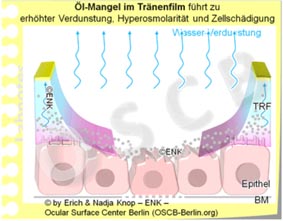
The Tear FILM has three layers constituted by the products of different glands. Mucins from single goblet cells (GC) in the conjunctiva make the surface wettable by the Water from the Lacrimal Gland. Oil from the Meibomian glands inside the eye lids forms the surface - it retards evaporation of the tear water and provides stability of the tear film.
A glimpse into the TEAR FILM. The main phase of the Tear Film overlying the transparent cornea is composed of the aqueous fluid from the lacrimal gland. Below are the numerous finger-like protrusions of the surface cells. Their cell bound and and loose secreted mucins (pink filaments) constitute the basal mucin layer that binds the tear water to the ocular cell surface. Mucins mix with the water and together they form a water-mucin gel. The surface of the Tear Film is covered by a very narrow oil layer from the-lipids of the Meibomian glands. The lipid layer has the same thickness and coloring as an oil film on a puddle of water. A main function of the oil layer is to retard the evaporation of the aqueous main phase of the tears. Consequently a lipid deficiency due to a dysfunction of the Meibomian glands is presently reported as the main causative factor for Dry Eye Disease.
What is the role of the Eye Lids?
=> They spread the essential pre-ocular Tear FILM !
This schematic animated diagram illustrates the principal eye lid function of tear spreading - actual tear drops occur in the palpebral fissure only during increased tear secretion.
The wiping movement of the upper eye lid during the blink spreads the tears into the thin and homogeneous Tear FILM.
This blink movement of the Eyelids is not only necessary for keeping the moisture of the tissue in the palpebral fissure ...
... but, at the same time, the tear film is the main surface for refraction of the light to provide perfect vision.
Another function of the blink is that the force of the lid muscle expresses some oil from Meibomian oil glands inside the Eyelids.
A lack of blinking therefore leads to a lack of oil on the tear film and to its instability.
In conclusion, the necessary prerequisites for a stable Tear FILM and thus for ocular surface health and visual acuity are SECRETION of tear fluid by the glands and the FORMATION of the tear FILM by the blinking action of the eye lids …
... consequently an alteration of Gland function and/ or of Lid function may lead to a Dry Eye condition - if this occurs chronically it may result in Dry Eye Disease.
In addition to spreading the Tear Film from the tear fluid, the eye lid action during blinking also contributes to the drainage of the ´used´ tear fluid via the lacrimal drainage system into the nose.
WHY is the Ocular Surface so important ?
=> The Healthy Ocular Surface is a Pre-Requisite for Vision !
The healthy Ocular Surface provides the clear window of the eye to see the light from the environment.
Without a healthy ocular surface all later steps of the vision process are meaningless.
Some DETAILS on Dry Eye Disease
DRY EYE DISEASE is an impairment of permanent moisture of the Ocular Surface with subsequent Destruction of the Tissue and a Reduction of Visual Acuity.
What IS DRY EYE DISEASE?
=> An Alteration of the Tear FILM that typically leads to Damage of the Ocular Surface Tissue
Dry Eye Disease is often termed as ´KeratoConjunctivitis Sicca´ (KCS) or simply known as ´Dry Eyes´, Burning Eyes, Itchy Eyes, Heavy Eye Lids, Tired Eyes ... and many other colloquial expressions that refer in one or the other way to ocular irritation.
Dry Eye Disease is a complex dysregulation of the functional anatomy of the ocular surface that impairs the permanent moisture and the integrity of the tissue and thus its health and the intact vision.
It typically goes along with signs and symptoms of ocular dryness, ocular irritation, tissue destruction and pain as well as with visual impairment, mainly in the sense of fluctuating visual acuity. and blurred vision.
WHAT are the CAUSATIVE FACTORS for Dry Eye Disease ?
=> A Deficiency in the PRODUCTION of Tear Components and/ or a deficiency in the FORMATION of a stable tear film are the main causative factors that lead to subsequent desiccation and damage of the tissue
Basic CAUSATIVE FACTORS for the pathology are:
- (1) a Deficiency of Gland SECRETION/ Tear PRODUCTION by any pathology of the ocular glands that leads to an insufficient quantity and/ or quality of tears and/or
- (2) a Deficiency in the FORMATION of a sufficiently stable Tear FILM from the available secretions, by any eye lid or blinking problem (termed as Lid- and Blinking Dysfunction - LBD).
The alterations in the function of the ocular glands and/ or of the blinking mechanism lead to INSTABILITY of the Tear FILM and thus to impairment of permanent ocular surface wetting. Insufficient wetting then results in DAMAGE of the Ocular Surface Tissue !
TYPICAL SYMPTOMS
in Dry Eye Disease
What are typical SYMPTOMS of Dry Eye Disease?
=> Typical subjective SYMPTOMS are various degrees of Ocular Dryness, Blurred Vision, Irritation and Pain !
The basic causative factors of insufficient secretion and/or insufficient tear film formation typically lead to SYMPTOMS such as::
- Dryness, grittiness, and foreign body sensation
initially, occasional episodes of increased tear flow and watery eyes can alternate with eye dryness
- Burning or stinging
- Irritation of varying degrees or pain
- Unstable visual acuity/ Blurred Vision
e.g. intermittent blurred vision that comes and goes and becomes better upon enforced blinking
- Moderate degree of eye redness
- ´Heavy´ eye lids or ´tired´ eyes or
- Contact lens wear is or becomes uncomfortable or impossible
Typical SIGNS
in Dry Eye Disease
What are typical SIGNS of Dry Eye Disease ?
=> Typical objective Clinical SIGNS of Dry Eye Disease are a reduced a reduced tear film stability and/ or tear volume on the ocular surface that reduce the moisture of the tissue and lead to surface damage !
A moderate DRY EYE typically shows only mild redness of the Conjunctiva and Lid Margins that indiates an inflammatory condition as described by the term ´Keratoconjunctivitis sicca´. The orifices of the Meibomian oil glands are often obstructed by visible or invisible inspissated secretum (which represents the most frequent primary cause of Dry Eye Disease). The tear volume is low and the tissue of the Ocular Surface epithelium has many small defects, that occur as small spots in vital staining with a green stain (fluorescein) observed in blue light.
The lack of sufficient tear fluid or of a sufficiently stable tear film that is often caused by a Dysfunction of the Meibomian Glands (MGD) results in respective pathological SIGNS: of the Eye Lids, Lid margins and Meibomian Glands as well as of the Tears, the Tear Film and of the Corneal and Conjunctival Epithelial Surface:
the tear film ruptures quickly and has a short ´break up time´ (BUT)
- this is typically evaluated by staining the tear film with a green stain (fluorescein) observed in böue light in order to make break-up of the tear film visible
- the animated schematic diagram to the right illustrates a highly pathologic tear film that is stable for only one single second - whereas a normal value should be at least ten seconds or longer (until the tear film ruptures and triggers another blink to reform a new tear film).
initially, occasional episodes of increased tear flow and watery eyes can alternate with eye dryness
there is a Low tear volume on the Ocular Surface
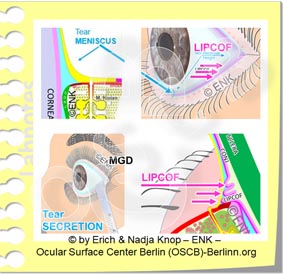
- this is detectable as a low tear meniscus height (TMH) and, more precisely, as a decreased radius of the tear meniscus curvature
- due to either increased evaporation of tear water due to a deficiency of oil secretion (this is the main primary reason - termed evaporative dry eye)
- or due to decreased secretion of aqueous tears from the lacrimal gland (termed primary aqueous deficient dry eye)
Deficient/ thin oil layer on the tear film
- typical consequence of Meibomian Gland Dysfunction (MGD) - the main primary cause of Dry Eye Disease
Lid Margin Alterations, such as:
- Meibomian gland orifices with pouting or plugging by inspissated material
- increased redness and increased blood vessels (teleangiektasia)
- foam and debris on the lid margin
- rounding and irregularity of the posterior lid border
Defects of the epithelial tissue that covers the Ocular Surface (Epithelial Vital Staining)
- of the Cornea and Conjunctiva
- of the Lid Margin as Lid Wiper Epitheliopathy (LWE)
Elevated levels of inflammatory mediators in the tears and tissue
- inflammatory cytokines, chemokines
- downstream activation of tissue degrading enzymes
Lid-Parallel Conjunctival Folds (LIPCOF) along the lid margin
- as a sign of tissue destruction due to activation of tissue degrading Matrix-Metalloproteinase (mainly MMP9) enzymes
Disappearance of Meibomian gland tissue (Gland Drop-Out)
- occurs in visualization of the glands by specific techniques (Meibography)
Pain Symdromes
in Dry Eye Disease
WHY are the subjective SYMPTOMS and the clinical SIGNS in Dry Eye Disease often disparate?
=> ... this is not completely clear as yet and still an issue of ongoing scientific investigations 1!
In Dry EYE DISEASE there is often a Disparity between subjective Symptoms of the Patient and the objective clinical Signs
In some cases intense subjective symptoms are causing a severe suffering of the patient whereas the clinical investigation may only observe few minor manifest alterations or even now pathology - this may probably point to a potential chronic pain syndrome.
On the other hand there may be a patient who in fact has severe objective alterations of the normal structure and function but does not suffer from any severe symptoms or may probably have no symptoms at all. Such a patient may then have only a limited interest in therapeutic interventions even though these may be very advisable from a clinical perspective.
The processing of signals from the Ocular Surface is complex and is influenced on different levels of the nervous system. Therefore, the outcome depends on many variables and may very well be different in different individuals. This fits well with the observations from our daily lives, that different people tend to have different ´nerve costumes´ and may react differently to the same stimuli.
Another issue is, that there is a principal difference between a ´perception´ e.g. of touch in a peripheral organ, such as the cornea, and something that we call pain.
PAIN is not a mere perception but is basically more of a feeling, because it contains an emotional aspect that the brain allocates to an incoming afferent impulse from the periphery.
The emotional aspect that the brain allocates to the stimulus is based on very individual things like previous experiences, recent emotions, or future expectations ... in order to name just a few factors. Therefore the actual feeling that is generated in the brain can vary to a large degree in different individuals. This may point to a neuro-biological possibility for explanation of the disparity of signs and symptoms in Dry Eye Disease.
Pain has the biological sense to alert us in order to avoid dangers that may threaten our health or our life. Under certain conditions when a pain becomes chronic and when it leads to a damage of the nervous system itself, it can develop into a chronic PAIN SYNDROME. Pain has then lost its biological function and becomes a disease of its own. In such cases where chronic pain persists without an identifiable tissue damage it may be useful to seek the help of a pain specialist.
L'influence psychosomatique sur un processus pathologique et sur sa propre perception par le patient est une partie bien établie et bien reconnue de la médecine à long terme. Mis à part par exemple la douleur dorsale, la dysfonction cardio-vasculaire et la dysfonction intestinale, une composante psychosomatique peut également jouer un rôle important dans la sécheresse oculaire, comme le confirment de nombreuses études. Lorsque la maladie devient la principale préoccupation dans la vie quotidienne, cela peut suggérer qu'il pourrait être utile de demander l'aide de psychosomatiques.
How do we GET Dry Eye ... and Why does it get WORSE?
How do we GET Dry Eye Disease ?
=> Dry Eye Disease is strongly influenced by Regulatory Systems and Risk Factors
Several factors influence the function of the Ocular Surface.
An impairment of positive factors and the occurrence of negative factors both decreases the normal function of the tissue and thus increase the likeliness and severity of a potential Dry Eye Disease.
The complex dysregulation of the functional anatomy of the ocular surface in Dry Eye Disease with a deficiency of the basic functional complexes for permanent moisture is influenced by different factors:
REGULATORY SYSTEMS
Failure of regulation
Failure of mainly the Nervous System, Endocrine Hormonal System, and the Immune System deteriorates the function of the Ocular Surface. Age and female Sex, related to a predominating estrogen action with relative lack of androgens, appear as the main predisposing factors for a higher risk of Dry Eye Disease
external Risk factors
mainly desiccating
Negative external influence factors represent RISK factors for disease. They influence the tears on the surface and can override the normal functional capacity. They mainly occur in desiccating environments, contact lens wear, visual tasks with low blinking frequency. Many occur combined in typical office work environments and may lead to a Dry Eye Condition termed "Office Eye".
internal Risk factors
Alteration of organ Health
Negative internal influence Factors represent RISK factors of the onset of disease. They act on the tissues that produce the tear fluid and can deteriorate the normal function. These are e.g. chronic diseases, chronic medication, age, sex, nutrition or hydration etc.
Why does Dry Eye Disease tend to GET WORSE ?
=> Tear Film Deficiency with decreased wetting of the tissue and Tissue Damage negatively influence each other in self enforcing vicious circles and lead to progression of disease !
Self enforcing Vicious Circles
The complex pathologic events in Dry Eye Disease tend to influence each other negatively and thus form self enforcing VICIOUS CIRCLES of Disease Progression.
This does often lead to a worsening of disease without a timely diagnosis and an effective therapy.
Inflammation is an important mechanism
Inflammation is an important mechanism for worsening of Dry Eye Disease.
Inflammation is a basic protective mechanism of cells and tissues against wounding and destruction, as typically occurs in Dry Eye Disease due to tear film instability and increased friction. Inflammation initiates destructive mechanism in order to overcome the ´destructor´ and is later followed by tissue repair.
When inflammation becomes chronic, however, it transforms into a negative and destructive process because the initial destruction can not be followed by a sufficient repair.
In chronic diseases like Dry Eye Disease, the chronic tissue wounding may lead to a chronic inflammation that drives some vicious circles and can thus greatly enhance the disease process.
Dry Eye Therapy to interrupt the vicious circles in Dry Eye Disease may then include an anti-inflammatory therapy for a limited time in addition to a sufficient Tear Supplementation and Eyelid Therapy .
For more detailed information on THERAPY in Dry Eye Disease please see the Full Length English Language Pages of the OSCB
.
When is a Dry Eye a ...DISEASE ?
WHEN does a "Dry" Eye turn into Dry Eye DISEASE ?
=> When ´Dry Eyes´ become chronic an occasional condition of ocular dryness can turn into a disease !
AN OCCASIONAL “DRY” EYE IS NOT YET A DISEASE
Most of us have probably already had an occasional sensation of a “dry” eye, e.g. when we are exposed to an unusually dry and desiccating environment, characterized by Low humidity, hot temperatures, high wind speeds and/ or by Low blinking frequency due to intensely concentrated visual tasks as e.g. in screen work
Such a “dry” eye is is typically a short-lived condition that disappears as soon as we become aware of it and remove the described desiccating stimulus.
WHEN “DRYNESS” BECOMES CHRONIC THE CONDITION TURNS INTO A DISEASE
Only when the feeling of “Dryness” remains constantly and cannot be removed or sufficiently improved by avoiding desiccating environmental stimuli and/or by improving blinking
… then the conditions becomes chronic and an occasional “Dry” Eye may develop into Dry Eye DISEASE.
This is typically related to an increase in duration and intensity of symptoms and by increasing severity of clinical findings/ signs due to increasing alteration and wounding of the ocular surface tissue
Several Different and Interacting self-enforcing VICIOUS CIRCLES of disease aggravation and worsening occur in chronic Dry Eye Disease and can lead to the full blown clinical picture with a progressive tissue destruction and a loss of function of the ocular surface.
