
QUICK GLIMPSE
... on the Ocular Surface, Dry Eye Disease & Contact Lenses ... together with some ideas for THERAPY

Choose your CHAPTER of Interest - or simply read along ... which may be most instructive
The Ocular Surface
The OCULAR SURFACE ... is the moist anterior part of the eye
The shining of the Ocular Surface comes from the Tear Film ...
... that maintains the permanent Moisture of the Ocular Surface.
The OCULAR SURFACE performs the first steps of VISION
The OCULAR SURFACE is that part of the eye that permits the entrance of Light.
Only after passing the Ocular Surface
... can this light elicit responses of the Retina in the back of the eye
... that later allow the ´curious´ Brain to construct an image of the outside world on the screen of consciousness.
Without a healthy and functioning Ocular Surface, all other steps of the Vision Process that happen later and further ´behind´ ... are basically meaningless.
The OCULAR SURFACE must be permanently MOIST
Our Ocular Surface has the biological requirement that it must be permanently moist - ´always and everywhere´ - to keep the transparent window of the cornea indeed clear.
The Moisture is produced by the associated Glands of the Ocular Surface and it is termed as the ´Tears*.
Since we are living in a dry environment with an air atmosphere, it is actually quite laborious to preserve this little artificial moist ´ecological niche´ of the Ocular Surface - ´always and everywhere´ !
PS: * except for moistening the Ocular Surface, Tears are also of use to give the emotional signal to our fellow human beings that we are exceptionally sad ... or probably exceptionally happy by shedding ´tears of joy´
Opening the eye lids for the entrance of light ... puts the Ocular Surface in some kind of a DILEMMA
The requirement of Moisture - ´always and everywhere´ - confronts the ocular surface with a problem or, more positively thinking, this gives it the change to deal with a Challenge:
Light can only enter the eye when the eyelids are opened ...
... on the other hand, opening of the eyelids would at the same time immediately deprive the Ocular Surface tissue of its moisture and it would start to dry out.
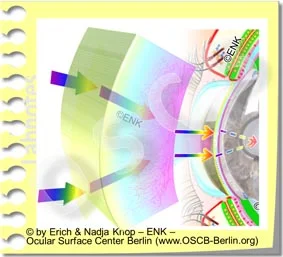
To solve this Dilemma, the Ocular Surface has to apply a ´Trick´: A very narrow layer of fluid is formed from the tears - this is for obvious reasons termed as the Tear Film.
The Tear Film is thick enough to preserve the moisture for the underlying cells of the tissue but not too thick in order not to harm the transmission of light.
The Ocular Surface in fact manages to be even more ingenious, because it solves the dilemma by even improving the passage of light through the presence of the Tear Film. The Tear Film fills in all subtle inequalities of the ocular surface and thereby provides a perfectly Smooth Surface layer for perfect refraction of the incoming light that allows for perfect Visual Acuity.
The TEAR FILM is the SOLUTION for all requirements of the Ocular Surface ... and for VISION
The Tears are transformed into the thin, homogeneous Tear Film through the coordinated Blink Movement of the Eye Lids.
During the Blink mainly the upper eye lid wipes over the anterior surface of the eyeball and thus distributes the tears into the Tear Film.
Only through the coordinated blink movement of the eyelids, together with the very special composition of the Tear Film, is it possible to form a Film that is extremely thin (only about one hundreds of a millimeter).
At the same time this very narrow tear film must still be stable to allow the curious brain to achieve a sufficiently sharply focused image of the outside world.
The Tear Film must be stable for at least 10 seconds on average until it eventually breaks up and triggers a stimulus that induces a new blink that forms a new tear film.
Having said this ... all major things are basically named ... The basic functional pre-condition at the ocular surface for vision is a Stable Tear Film. This is achieved by the Basic Functional Complexes of Tear Secretion/ Production by the ocular glands and of the physical Tear Film Formation by the blink movement of the eyelids.

Dry Eye Disease
. . . ´After the MOIST is gone´ . . .
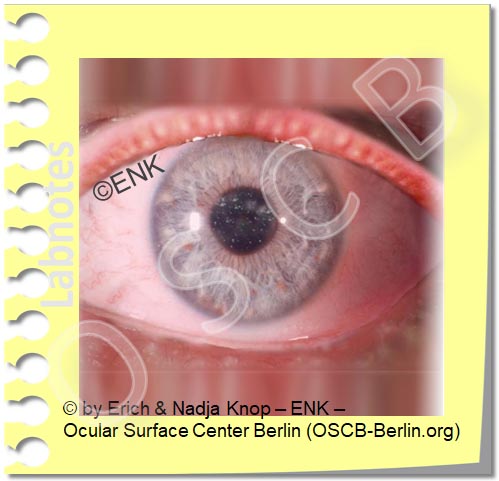
IF NO (sufficiently) stable Tear FILM is present ... this will eventually result in a DRY EYE.
Because the formation and preservation of the Tear Film is very laborious in the dry environment that we live in, it is very failure-prone.
The Tear Film is influenced by a multitude of very different Influence Factors and Risk-Factors, that can, in one or the other way, have a negative influence on the Tear Film.
ALL these negative factors can, sooner or later, lead to a Dry Eye condition. The large number of influence factors that may appear unrelated at first glance can let Dry Eye Disease appear as a ´Tricky Condition´ - even though it basically straightforward.
The fact that the Tear Film is there to prevent Drying of the Ocular Surface Tissue indicates that typically the most immediate consequence of a Dry Eye condition is the Drying and thus Destruction of the Ocular Surface Tissue.
This results in a ´downstream´ irritation of nerve fibers that transmit ocular irritation of various degrees probably leading to a chronic pain syndrome, and inflammatory reactions that can reinforce the whole process.
Since the Tear Film also has an important function for the refraction of light and thus for the provision of visual acuity, it is no surprise, that visual disturbance is frequently reported in Dry Eye Disease, typically in terms of unstable visual acuity and blurred vision
Some Ideas for THERAPY in Dry Eye Disease
What can be done as a THERAPY for Dry Eye Disease ?
In most cases there is a deficiency of the Tear FILM based on a qualitative or quantitative lack of Tear Components.
Therefore TEAR SUPPLEMENTATION, i.e. the addition of missing tear components - in the form of eye drops or of a spray - is the most frequently used therapy option.
Sometimes this is termed Tear ´Replacement´ - but, since the (full) Tears with all ingredients can (unluckily) not be replaced at present and in the foreseeable future, the term ´Supplementation´ appears more appropriate.
All different sorts of eye drops based on aqueous solutions with a lot of different additional ingredients are available, mostly as prescription free over the counter products.
A lack of OIL is the main starting point for Dry Eye in most patients with Dry Eye Symptoms
According to the present scientific knowledge, the vast majority, i.e. four of five patients with a Dry Eye Condition, does NOT have a primary lack of water but instead a PRIMARY LACK OF OIL in the tear film.
This leads to increased water evaporation and decreased tear film stability .... with a secondary water loss.
Therefore, in most patients, it does not seem to make much sense nowadays to use products that do not contain lipids in one or the other way.
It may be possible to replace the effect of lipids on the tear film by other compounds, or to simply use lipids only, e.g. as a liposomal spray. ... In other words, LIPIDS or respective compounds should nowadays be a component of a typical Tear Supplementation Therapy.
The lack of oil is typically due to a Dysfunction of the Meibomian Glands inside the Eyelids.

The lack of oil on the ocular surface is typically due to Meibomian Gland Dysfunction (MGD), a mostly obstructive condition of the Oil-producing little glands inside the eye lids.
The glands are blocked by inspissated secretum and excessive keratinization - therefore inspissated oil accumulates inside the glands.
Muscular force during blinking of the eyelids normally helps to express the oil from the Meibomian glands.
Rare Blinking is thought to be an important factor for a lack of oil on the tear film and possibly a co-factor for onset of gland dysfunction.
Intended forceful blinking is known as a simple way to increase the oil layer on the tear film and thus to improve tear film stability in order to prevent ocular surface dryness.
Physical EYELID Therapy
PHYSICAL EYELID THERAPY is reported to restore the function of the Meibomian glands in the Eyelids ... and thus improves Dry Eye Disease
Physical Eyelid Therapy options refer to the fact that the improvement of Eyelid and Meibomian Gland Disease is based on simple but effective physical techniques such as Warming and Moistening, as well as manual Massage and Expression of the Glands with subsequent Scrubbing and Cleaning of the Eyelid Margin.
It is certainly important to note that before any manipulations are done to the eyelids and the eye a clinician should always be consulted for an educated diagnosis and for therapeutic recommendations !
Physical Therapy should be done as a permanent therapy, at best twice a day, because a chronic disease typically requires a chronic therapy !
Physical Therapy consists of 3 Steps
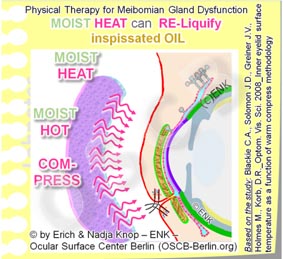
(1) WARMING of the Eyelids
- WARMING, preferably together with moisture
- for at least 10 minutes
- to reach a temperature of 40°C inside the eyelid and thus within the Meibomian Glands
- serves to re-liquefy the inspissated oil inside the Meibomian glands.
In order to achieve 40°C inside the eyelid a slightly warmer (42-45°C) moist warm compress/ cloth must be rewarmed (e.g. from a larger bowl of hot water) every two minutes as shown by studies.
The additional moisture serves to soften up the cornified epithelial squames and lipid encrustations on the eyelid margin.
Commercially available gel masks of even electrically heated and moistened googles may make the potentially laborious effort of physical therapy, twice a day, considerably easier ...
(2) Subsequent Lid MASSAGE to EXPRESS and relieve the obstructed glands
- when the inspissated oil that is stuck inside the Meibomian glands is sufficiently warmed it will become more liquid again
- a careful eyelid massage can then express the pathologic content from the Meibomian glands onto the lid margin
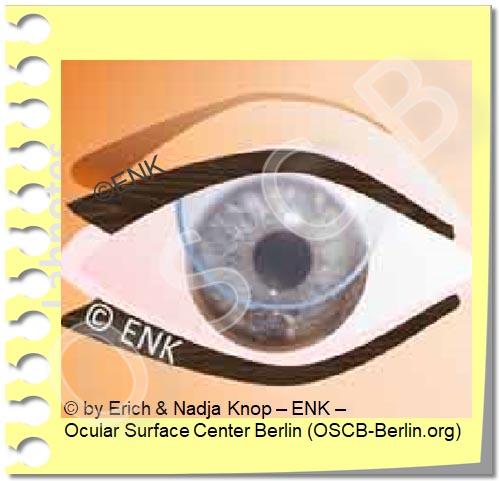
- massage must always be directed towards the gland orifice on the lid margin, i.e. towards the palpebral fissure (as shown in the animation to the right)
- the upper eyelid is thus massaged downwards
- the lower lid is massaged upwards
- when the oil is very hard and insufficiently re-liquefied it may be necessary to perform a more vigorous expression of the eyelid , e.g. between two fingers
- this can potentially hurt the eyelids and glands
- during any procedures applied to the eye by a layman it must therefore alway be safeguarded that no harm and wounding is caused to the eye, eyelids and glands !
(3) Eyelid/ Lid Margin HYGIENE concludes physical therapy
- finally, the eyelid margin together with the base of the eyelashes could be cleaned
- from the expressed pathological oil
- from bacteria and bacterial products that occur on every normal lid margin but increase in disease
- from cornified skin squames that deposit on the lid margin
- Lid Margin HYGIENE can be done by a soap-free wiping or ´scrubbing´ of the lid with a cotton-tipped rod or a cosmetic pad in order to remove any debris, encrustations and foam from the lid margin.
- it appears important to avoid any soap, shampoo, or any other detergents, as has previously occasionally been recommend., because that would conceivably harm the tear film lipid layer.
- Oily solutions of any kind appear more suitable for eyelid cleaning.
- Commercial eyelid cleaning kits are available that contain everything necessary in a pre-prepared set and may make eyelid hygiene much easier.
The advantage of such physical therapy options is certainly, that this can mostly be done at home by the patients themselves. It may appear as a disadvantage that physical therapy and in particular lid hygiene has to be done routinely once or twice a day, similar e.g. to tooth brushing, but requires slightly more time.
Please Remember: A Happy Eye Lid typically makes a Happy Dry Eye Patient !
... or, to re-phrase it in the Roman way: ´palpebra sana in corpore sano´ - unproven quote from Clarissimus GALEN ;-)
- - -
Various other THERAPY OPTIONS are discussed in other Chapters of the full length English Language Pages of the OSCB Information WebSite.
Contact Lenses
CONTACT LENSES are a fantastic Optical Tool ... customized to the Ocular Surface
Contact Lenses are a fantastic Optical Tool with some clear optical advantages compared with spectacles.
At the same time they provide greater ´freedom´ for outdoor activities, sports and society events.
Contact Lenses are, as their name indicates, in direct ´contact´ with the Ocular Surface.
Contact Lenses are in fact sitting in the middle of the Ocular Surface Functional Unit - with potential influence on all tissues and on the tear film. Contact Lenses thus have a somewhat ambiguous role for the Ocular Surface - with Pros and Cons.
Contact Lenses are swimming on the Eye ... and thus have higher requirements for the Tear Film
Contact Lenses can be used for medical purposes such as the optical correction of an irregular corneal shape or for the protection of the eye e.g. in severe cases of Dry Eye Disease.
On the other hand, Contact Lenses have higher ´requirements´ for the amount and/or quality of the tear film.
It may well be, that an individual with a borderline normal tear film, who is still without symptoms, may develop Dry Eye symptoms upon insertion of an ordinary soft hydrogel contact lens. A typical side effect of Contact Lenses is therefore the onset of Dry Eye symptoms and eventually probably of Dry Eye Disease.
On the other hand an individual with a severe Dry Eye Disease may profit from the application of a special so-called ´Scleral´ Contact Lens that is able to preserve the tear solution underneath the contact lens and in front of the cornea.
HYGIENE is a CRITICAL ISSUE in Contact Lens Wear
Contact Lenses have seen great improvements in the past decades.
This has lead to a reduction in the frequency and severity of side effects.
Insufficient Hygiene can lead to serious and sight-threatening infections in contact lens wear.
This is still an important issue, particularly for inexperienced wearers.
Due to the increasing use of disposable contact lenses for short term wear, particularly daily disposables, the risk of infection can be reduced.
Please find more information below on => Contact Lenses and the Ocular Surface
